




In his competition winning article posted on August 23rd 2018, Major Richard Ward, Officer Commanding (OC) B Squadron (5th Aviation Regiment), outlined some of the aeromedical evacuation (AME) capability enhancements which were showcased on Exercise Hamel 18. We commend him for his personal drive and commitment to be part of the collective movement to offer solutions to some of the challenges for the Australian Defence Force (ADF) casualty evacuation (CASEVAC) continuum. The author is rightly proud that medical technicians and medical officers on Ex Hamel were able to demonstrate CASEVAC from a simulated non-permissive environment. In particular, these activities were undertaken without some of the constraints that have hampered AME operations since the introduction of the MRH90. For example, the medical attendants were able to treat casualties without being confined to their seats – previously routine business on ADF Blackhawk AME missions. Other modest developments in personal equipment, communications and procedures that have been ‘a work in progress’ for the past few years were also showcased on Ex Hamel.

His article aims to discuss the broader ADF capability gaps within the Forward and Tactical CASEVAC domains. We contend that despite the best intentions of the teams preparing for and conducting ‘Combat Recovery’ operations during Ex Hamel, there is indeed a very long way to go in the development of the entire CASEVAC system. Air Commodore Tony Austin wrote in 2002 that '…as the performance (and cost) of the equipment and aircraft increases, it is imperative that the training of military AME team members is improved. As it is, the skills of AME personnel in the Australian Defence Force threaten to be the weak link in the chain.'[1]
Our view is that relatively little has changed in the ADF since this comment was made, and indeed little has changed in Forward ADF AME since the DUSTOFF missions flown during the Vietnam War era. It remains the case that the skills of the personnel in the ADF CASEVAC chain need greater focus and development. We believe that a true paradigm shift is required before the ADF will actually have anything to celebrate in the Forward and Tactical CASEVAC continuum, including the AME component of that continuum. But we do agree that a “world class capability” is achievable as suggested by Major Ward. We propose the Sea, Air, Land Treatment and Transport (SALTT) model as part of a comprehensive reconsideration of CASEVAC in the ADF.
Why the need for a rethink?
The landmark Eastridge et al[2] analysis of 4,596 battlefield deaths between 2001 and 2011 during the Afghanistan and Iraq campaigns revealed that almost nine out of ten (87.3%) combat deaths occur prior to arrival at a medical treatment facility (MTF). Of concern, analysis of those deaths revealed that almost one quarter (24.3%) were potentially survivable. Conversely, a patient arriving ‘with a pulse’ to a modern military hospital with surgical and advanced medical capabilities has up to a 98% chance of surviving.[3] The clear implication is that any significant future gains in battlefield survival must be made in the pre-MTF domain. While the general focus is understandably on improving survival (mortality), it is recognised that for every person who dies, there are between four and six severely injured. Perhaps therefore an equal, if not bigger, focus should be improving ‘final functional outcome’ (morbidity) for survivors.
As Captain (Dr) James Savage points out in his article for The Cove, the current model of care in the ADF for rotary-wing AME (RWAME) is inadequate for complicated battlefield casualties. The modest capability improvements witnessed during Exercise HAMEL 18 are not enough. The somewhat romantic notion that a patient can be ‘saved’ so long as we just ‘scoop and run’ and get to a first-world military hospital, with little meaningful intervention en-route, is not borne out in reality. It is akin to suggesting that a scrambled egg can be put back together so long as we get quickly to the world’s best chef! This belief is reflected in the core philosophy of sophisticated pre-hospital systems that believe 'exceptional ‘downstream’ care will never compensate for a relative denial of ‘upstream’ care’.
Captain Savage is correct when he says that we need to train and develop retrieval teams for the ADF that can effectively treat critically injured patients from the point of injury. He introduces SALTT teams as a potential ‘game-changer’ in the scenario he developed. Important decisions, such as diversion to an alternative MTF (e.g. Shock Trauma Platoon, as described in his vignette) are best made by experienced critical care clinicians. Safe CASEVAC of those patients within the Area of Operations (i.e. Forward and Tactical) will necessitate significantly more highly trained and equipped teams than the ADF can currently deliver.
Why is it so important to improve our entire CASEVAC system?
The experience from both civilian and military trauma systems tells us that patient outcomes are better when the patient is transferred to an appropriate medical facility. It is well established in civilian trauma systems that it is often better to bypass small, provincial health facilities in order to transport to a centre that is definitively able to address patient needs. A patient suffering serious traumatic injuries will never be delivered to an urban General Practice, for example, no matter how close it might be. The ambulance will transport the patient to the ‘trauma centre’ because we know that bypassing some smaller medical facilities will ultimately reduce the time to appropriate treatment for the patient. This is also true in military trauma. We bleed the same blood. We need the same level of care!
In contrast military CASEVAC plans often involve sequential echelons of care as implied with the ‘10-1-2’ paradigm (10 minutes to enhanced first aid, one hour to advanced resuscitation and two hours to damage control surgery). A typical patient journey is planned to proceed from a Role 1 (R1 = primary care and basic resuscitation), to a Role 2 (R2 = initial damage control resuscitation and surgery) and rearwards to a Role 3 (R3 = definitive and subspecialty surgical care) facility. However, as with the civilian experience, the military literature tells us that some patients will have better outcomes if they bypass the R1 (and sometimes the R2, depending upon the needs of the patient and the capability of that R2) to proceed to a MTF able to deliver higher levels of care[4],[5]. The ability to provide advanced clinical judgement and enroute resuscitation is therefore a vital part of the journey, especially if the journey to the medical facility is more than a few minutes.
CASEVAC is more than a simple logistics function of delivering a patient to the nearest MTF. Future improvements in the ADF’s CASEVAC systems, especially in the Forward and Tactical environments, must focus on improving the skills and training of the medical personnel involved. Also, discussions need to move beyond RWAME. We acknowledge that RWAME will remain a vital capability into the future, but our system cannot rely solely on the availability of RW CASEVAC assets. Also, they may not always be suitable for CASEVAC in future military operations where air superiority is not guaranteed. We must build our CASEVAC system with the ‘worst-case scenario’ in mind. This mindset is routine thinking for military operations and it should be the same for military medical planners.
What is ‘SALTT’ and why is it an important part of the solution?
SALTT will be a tri-service, multi-disciplinary team capable of delivering critical care in Forward and Tactical CASEVAC utilising any transport platform. The selection, training, and equipment of SALTT teams will enable them to be utilised in non-permissive as well as permissive environments. The only existing ADF critical care CASEVAC capability is the RAAF Military Critical care Aeromedical evacuation Team (MCAT). However, MCAT is unsuitable for Forward and non-FW Tactical CASEVAC due to their operational mindset and training, and personal protective and medical equipment being poorly suited to that role. In recent decades the ADF has relied on coalition partners or contracted civilian agencies to fill this Forward and Tactical CASEVAC capability gap.
It is intended that SALTT teams will be highly selected from the outset, with a rigorous and competitive process for choosing individuals with the right personal, as well as professional, attributes. Each three-person team will comprise one critical care physician, one critical care nurse and one paramedic. They will be drawn largely from the ADF reserve forces because they will need to actively work in critical care disciplines and retrieval medicine in order to maintain their currency and proficiency. The equipment and posture of this team will enable them to safely treat and transport critically unwell patients by day and night on a range of rotary wing, fixed wing, land surface and seaborne transport platforms in both permissive and non-permissive environments. As might be expected, SALTT teams would be particularly suited for supporting amphibious operations.
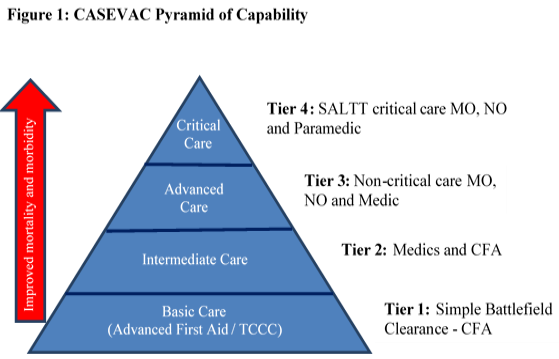
The vision for the SALTT teams goes beyond their crucial role for the treatment and transport of very seriously injured or ill patients. We propose that SALTT should be viewed as the ‘tip of the pyramid’ for ADF CASEVAC capability (Figure 1). SALTT teams will become a repository of technical expertise and would assist with enhancing the lower tiers of CASEVAC capability by delivering training, developing relevant SOPs and TTPs, identifying and testing innovative medical equipment and interventions, and by providing credible supervision and governance for the entire system. SALTT is not proposed as a panacea for the ADF CASEVAC system, or indeed a replacement for any existing capability. However, we believe SALTT should be seen as a vital part of a substantial CASEVAC system overhaul.
The ADF is currently unable to rely on its own resources for safe and effective CASEVAC of critical care patients outside of FW Tactical and Strategic AME. It is time for a substantial revision of ADF CASEVAC capability in the Forward and Tactical sea, air and land domains. We propose SALTT as a cornerstone capability for this revision. In his essay, Major Ward reminds us that we must not lose '…focus on what truly makes an Army great: its PEOPLE'. We agree! We must have people who are capable of doing the job. For critical care CASEVAC this means people who are appropriately trained and competent in critical care. We further assert that any review of CASEVAC systems within the ADF must look well beyond just RWAME teams. We need teams capable of transitioning seamlessly between sea, air and land platforms thereby enhancing operational robustness and flexibility. If the ADF is willing to invest in the high-end capability from the outset, the rest of the ‘CASEVAC pyramid’ will see immediate flow-on benefits. So too will the men and women of the ADF should the ‘worst case scenario’ unfold in ‘the next war’.




Roger stated that the ‘golden hour’ was something that his team always strived to meet, but it was not always possible due to staff assessment of the risks to retrieval assets. Specifically, the risk of loss of a helo, pilot, co-pilot and medical support staff was greater than the loss of a combat soldier. The key to enhancing survival pending casevac is immediate first aid and pain relief. It would often be many hours before a casualty was able to be recovered but most, not all, survived.
Given that casevac assets will be targeted by threat forces, it follows that soldiers must be capable of rendering advanced first aid in-situ until it is safe for a casevac extraction to be conducted.
As we review AME within the ADF, perhaps we should also review soldier training with a view to ensuring that a soldier knows as much about combat first aid as he does his field tactics and weapon systems in order to keep the clock ticking beyond the golden hour, depending on the threat situation. Clearly, there is a significant training liability involved here but the reality is, the threat force will target us to injure and maim knowing that his next targeting opportunity will be an AME extraction team. This enemy tactic can be assured given his likely knowledge of our ‘golden hour’ SOP.
Roger made me aware of an Emergency Care paper co-written by three British RAP medics and this may be instructive in any review. Certainly, the experiences of UK forces in Afghanistan would offer useful input for the ADF’s consideration.
Especially considering how advanced paramedicine has become in Australia compared to some other parts of the world, it would be great to tap into that workforce and bring such a forward critical care role to ADF capability.
Will be curious to see how CASEVAC evolves in future conflicts and how the reliance on more advanced in-field 'buddy-aid' and or more timely professional intervention develops.
detailed options for battlefield cas treatment
The Bankstown HEMS base is the largest and most complex Helicopter Emergency Medical Services base in Australia, and one of the biggest in the Southern Hemisphere.
The Bankstown base also includes the Aeromedical Crewing Excellence (ACE) Training Centre, a world-class training facility with highly realistic mission simulation technology for all aeromedical crew members.
The purpose-built centre includes specialist medical training rooms and helicopter simulation technology such as the Helicopter Underwater Emergency Training pool, a virtual reality training system and full flight AW139 simulator.
The base has at any one time, three dedicated AW139 rescue helicopters and two Road Retrieval Ambulances operating 24/7. These platforms consisting of Critical Care Paramedics (CCP) and Doctors who can deliver the same level of care to critically ill or injured patients.
Additionally, the helicopter medical teams consist of an experienced Paramedic who is Special Casualty Access Team (SCAT) qualified. The doctors are specialists in emergency and intensive care medicine and anaesthetics or are senior trainees in those specialties with a specific focus and enhanced training in pre-hospital and retrieval medicine.
During the last 20 years co-ordination between HEMS and the ADF have focused on four main areas:
1. Clinical placement with AME qualified medics conducting ride-along with both helicopters and road response ambulances.
2. Medical trauma training involving CCPs discussing trauma cases and training medics in advanced medical procedures.
3. Mission specific medical and aviation training involving CCP and doctors conducting mission specific training for Special Forces medics deploying to East Timor and Afghanistan.
4. ADF medics and doctors attending Ambulance Aviation medical, rescue and SCAT courses.
The aeromedical medical team induction course is a two week course designed to train doctors and paramedics to work together in a multi-disciplinary team while conducting their clinical care in an aviation environment. Doctors complete a further two weeks of training in aviation ground and flight school, including winch training to become Medical Transport Specialists. Helicopter Paramedics go on to complete another eight months of training in remote area access (SCAT), down-the-wire rescue crew and rescue swimmer training.
The remote area (SCAT) course is an eight week intensive Clinical Access Course for CCPs which involve all aspects of accessing patients including; vertical access, swift water rescue, helicopter familiarisation, canyon rescue, caving, four wheel driving and ocean rescue.
The ongoing success of the ADF and HEMS is largely due to the efforts of the head of Helicopter Operations,
Chief Superintendent Cameron Edgar (formerly a member of 1 Commando), who has continually taken an interest in progressing ADF and HEMs AME capabilities.
After 20 years the relationship between NSW Ambulance and the ADF is stronger than ever, with many opportunities. With the long-standing AME relationship combined with recent joint operations in support of bushfires and floods, there is more being looked at to enhance current ADF aeromedical capabilities into the future.
Chief Supt Edgar greatly values the relationship, as well as the ability to share and learn from Army to continually evolve best practice aeromedicine. “While we are share what we can from an equipment and procedures perspective, it is the networking and providing ADF medics with real-world experience and lessons that counts. We hope to continue this well into the future.”