




I have seen and heard the term ‘best practice’ used many times throughout my time in Army. When I hear the term being used, it is usually followed up by thoughts such as:
- How is it the best?
- Best practice according to whom?
- What was excluded from their definition of ‘best’?
It seems obvious no one would want to choose ‘worst practice’ and so there is use for this term ‘best practice’ to indicate that the person conveying the message truly believes it to be ‘the way’ to do things. However, to me this term is vague and unhelpful as it doesn’t provide any justification, references, or reasoning. While I don’t dispute the good intentions of those who use the term, I would like to promote a shift in both terminology and practice.
‘Evidence-based practice’ is a term that has been used for several decades now, particularly in health industries. The model below depicts the E3BP approach (Dollaghan, 2007), one of several models and one of the most well-known.
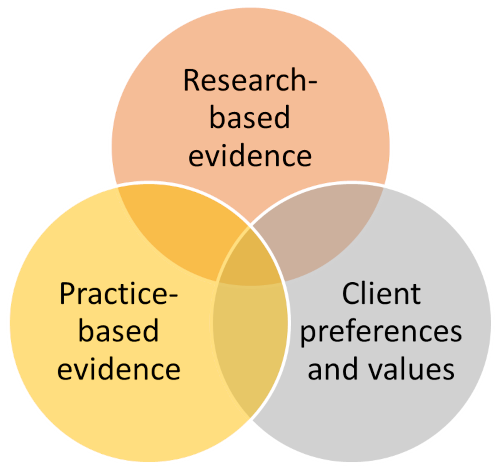
There are 3 highly integrated and equally important components to E3BP:
- Research-based evidence – the best available evidence from systematic research which holds high validity and is peer reviewed.
- Practice-based evidence – “technical expertise” (clinical expertise in the medical field) and evidence internal to the technical practice. Evidence collected in a technical setting which has greater life-application than that of some restricted research studies. Usually defined as a professional field e.g., medicine, nursing, engineering, education, etc.
- Client preferences and values – how the technical expert develops a shared understanding of the clients’ beliefs, preferences, and values so that they can be used to select goals, interventions, and targets that the client will have confidence in and comply with. The client may be an individual, a group of people, or an organisation.
Why use EBP?
EBP is a comprehensive approach to solving a problem in that it reviews quantitative research, incorporates real-life experience from the context, and it integrates the client’s perspective and their preferences and values. Including the client in the solution means their perspective is taken into account and allows them to see what the evidence says and how it should be applied. Clients need to be well informed in order to make good decisions.
The research base is constantly growing and so there is a need to engage in the research regularly. Reading one or two articles does not provide an individual with a large enough knowledge base to understand the research and to be able to judge it for reliability and validity (necessary skills that go beyond the scope of this article).
Just because new research comes out doesn’t mean that older research should be discounted. It needs to be critiqued and – depending on the problem or issue at hand – older research may be more applicable, especially if the client’s preferences dictate it.
Equally, there is an opportunity to conduct research within the organisation through appropriate research methodologies. Quality quantitative research will only benefit EBP within Army.
Experience in contexts is important and provides relevant evidence but it is not the only evidence that should be relied upon. It should help inform the solution, just the same way that empirical research and client preferences do – all equally. When using EBP there is no start point or end point as it isn’t a process. Instead, all components should be considered simultaneously as they interact heavily with one another, and all are equally important.
Who should use EBP?
While I advocate for EBP to be adopted across Army, Specialist Service Officers (SSO) are well placed to integrate EBP into practice because they come into the organisation with technical expertise; some have many years of experience in their fields, and they have a solid understanding of the research base. Many are members of professional bodies which also means that they keep in touch with the current research evidence base. Many in the medical and health fields will already be implementing EBP into their practice.
EBP as a model of practice is something that is continually done. Thus, even if a particular intervention or decision is made now, it doesn’t mean that it will continue to be the ‘best’ solution into the future. This is because the client’s needs shift, the research evidence base is continually developing, and technical experts gain more experience over time; therefore, the inputs into EBP change.
The ‘client’ will always be Army just at different scales (individual, sub-unit, unit, organisation) and this is where every member of Army has an important role in EBP. They can put forward their preferences, their needs, and what they value in a solution which will help to influence the direction while the technical experience and research will also provide guidance.
Thus, EBP does involve aspects of collaboration and integrated practice. For commanders and those in positions where decisions are to be made that involve different fields, such as training and education or engineering, it is important that they understand EBP as a model of practice that seeks the best possible outcomes for the client from the best available evidence, and it is not shrouded in any internal biases or personal opinions.
What does this look like in practice?
Example – Training for a sporting event
A group has recently signed up to an endurance sporting event to be held in a few months’ time and are looking to train so that they can finish the event with a personal best. The group has varying strengths and difficulties but are all committed to the event and so will complete whatever training is necessary. The group leader researches into training approaches for the same type of endurance sporting events (research evidence).
Two of the group members who have completed similar events in the past review their previous experiences and share them with the rest of the group (practice-based evidence). The group discuss what their goals for the event are, any existing injuries, medical needs, and preferences for training (client preferences and values).
Example – application to Army’s training context
As part of a new capability being introduced into service, a training strategy and learning solution needs to be developed. A review of research into training approaches of this type of capability as used by other militaries is conducted (research evidence). Current and previous training strategies and learning solutions in Army are reviewed for relevance, validity, and applicability to the new capability training (practice-based evidence). Consultation with the client: training establishment, school, and unit(s) to gauge their preferences and their values to be considered.



Great article (Linked-in) & on point. My MSc Security & Risk Management dissertation (2022) addressed this issue in part within the context of event security & counter terrorism. As a former ADF officer, it is very encouraging to follow the next generation of hybrid warriors - evidence based & practice based !
Yours aye,
Peter Ashwin