




The rock face into the village of Efogi 2 is not really a climb at all. It feels like a waterfall you happen to be climbing – in the rain, with a heavy pack, on the fifth day of trekking the Kokoda Track. Somewhere below it, the track gives up pretending to be a path and becomes water, rock, and tree root.
You go up because there is no version of this where you go back.
Picture a group of trekkers climbing over its lip, soaked through and muddy to the knees. Excited voices reach them through the rain: villagers waving from under their huts, out of the weather. It was a moment repeated, in some form, for more than 80 years: tired Australians coming up that waterfall into a village that has been welcoming them since 1942.
Somewhere not far off, an aeromedical evacuation helicopter punches across the sky – the sound of a casualty timeline familiar to anyone trained for expeditionary operations in dense, mountainous rainforest largely unchanged since the 1942 Kokoda campaign.
The Trek and the Cause
In April 2026, an 18-strong team walked the Kokoda Track in Papua New Guinea (PNG). This trek was completed over eight days as a fundraising expedition, raising more than $170,000 for the Commando Welfare Trust (CWT). They walked for the cause, for themselves, and for the soldiers who fought across this ground in 1942 – and across tracks like it around the world.
Those purposes were inseparable.

The CWT was founded in 2010 in the aftermath of devastating Australian Special Forces casualties in the Middle East. Its mission is plain: to provide a perpetual safety net for Special Operations Command soldiers, veterans, and their families – emergency and long-term financial support where existing systems cannot reach.
In the fifteen years since, the Trust has delivered over $7 million in direct support to more than 140 veterans and their families and currently supports 50 families including the children of fallen and wounded Special Forces members.[i]
The Trust exists because of more recent operations, but the ground that Kokoda crosses is the ground on which the Australian Defence Force first learned what it costs to fight in country like PNG. Walking the track for the families of one generation of Special Forces, on the ground that took so many of an earlier one, is its own form of continuity.
The expedition included an embedded health clinician, with kit and knowledge built around the predictable problems of dismounted operations in tropical mountain country. Across eight days of close clinical observation in realistic conditions, the trek demonstrated that these predictable problems are not new.
The diggers of 1942 met these problems with much less than is available today, and contemporary expeditionary health planning can learn from the comparison in ways no doctrine document can replicate.
The kit has changed; the physiology has not. What follows is what the ground had to say.
Hydration and Electrolytes
In 1942, the diggers could not get enough water. Resupply was sporadic, watercourses were not always potable, and the physical demands of sustained combat in steep, humid, tropical mountain country generated fluid losses that outstripped what soldiers under fire could replace. Dehydration was a constant factor in combat ineffectiveness across the Kokoda campaign.
A trekker in the CWT group faced the opposite problem. He had arrived in Papua New Guinea directly from five weeks in a cold climate and was drinking multiple litres of water a day on the track. By day two, he showed several signs and symptoms of acutely low sodium: nausea, headache, dizziness, lethargy, mild confusion, and muscle cramping.
He was managed with sodium replacement, fluid restriction, and overnight monitoring. He recovered. The contrast was striking: the same physiology and the same mountain, but opposite ends of the same curve.
The lesson is not simply that modern trekkers face low sodium where 1942 soldiers faced dehydration. It is that tropical operations are electrolyte problems as much as water problems, and that modern over-correction is its own clinical risk.
Pre-deployment health briefs that emphasise hydration without equal attention to electrolyte balance can set soldiers up for a different version of the same physiological failure. The diggers’ problem was the inability to access water. The modern problem is access to water without commensurate access to salt. Both endpoints are dangerous, and both are predictable.
Sustainment and Nutrition
Captain Tom Grahamslaw, who served on the track in 1942, recorded eating up to 2.3 kilograms of unsalted sweet potato a day to maintain function.[ii] That was the sustainment available. That was what kept him going. The caloric arithmetic of fighting and walking through that terrain demanded extraordinary intake of whatever could be carried, foraged, or supplied, and the diggers’ weight loss across the campaign is one of the better-documented features of the historical record.
After one particularly gruelling twenty-kilometre day, the CWT trek group were served a steaming bowl of locally grown sweet potato mash. Someone produced a shaker of salt, and it was passed around the table like a sacrament. Now try to imagine 2.3 kilograms of unsalted sweet potato a day… every day… while being shot at. It is not easily imagined.
Modern operational ration packs are calorically engineered, palatable enough to encourage consumption, and supplemented with electrolytes and protein. They are an enormous improvement on what 1942 could deliver. They have not, however, solved the underlying problem: caloric deficit on multi-day dismounted operations in mountainous country is almost certain, and it degrades performance, decision-making, and resilience in ways that current doctrine can still under-recognise.
Soldiers do not eat enough on operations like this. The lesson is that sustainment of the individual soldier is a force-preservation issue, not a logistics afterthought, and that any plan that assumes ration adequacy without attention to actual consumption is repeating a 1942 mistake with better food.
Foot Health
Foot conditions added to the heavy toll of disease and non-battle injury across the Kokoda campaign. Boots that never dried out, prolonged immersion in wet mud, fungal infection, trench foot, blisters that became cellulitis: these conditions removed soldiers from the line as effectively as enemy fire, and their effects compounded across the duration of the campaign.
Across eight days, the CWT trek group were offered glimpses into what the diggers had endured: blisters, rashes, friction wounds, and the early stages of trench foot. Each night the group hung wet boots and clothing by the fire and woke to put them back on damp the next morning. The phrase "boots that never dried out" went from a historical quotation to a daily reality.
With Owens' Corner in sight on the penultimate day, a trekker from another group was carried out with severe trench foot, advanced enough that weight-bearing was no longer possible. The terrain, the moisture, and the mileage had caught up with her.
The lesson is one that Australian Defence Force expeditionary health doctrine has been trying to reinforce for decades, and that walking the ground reinforces with unusual clarity: foot conditioning, footwear selection, sock rotation, and active foot care are not personal hygiene matters. They are clinical interventions with direct operational consequences.
Pre-deployment foot conditioning should be planned and resourced as such. The diggers learned this through experience. There is no need for a modern force to relearn it.
Casualty Evacuation
The trekker with severe trench foot did not get a helicopter. The local porters cut down trees. They used machetes. They lashed the logs together with what they had, and eight of them carried her out, multiple kilometres, over tree roots and rock, through water crossings, both uphill and downhill.
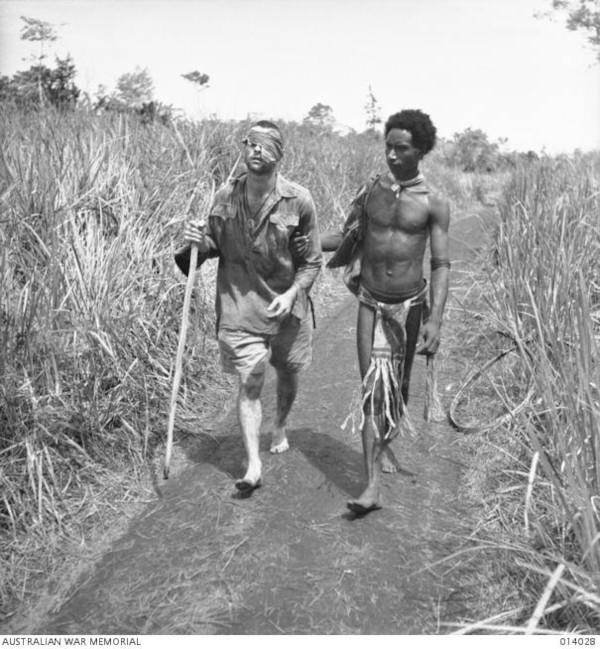
Anyone who has read about Kokoda has seen George Silk’s photograph of Private George Whittington being led through the long kunai grass by Raphael Oimbari at Buna in late 1942 – the image most closely associated with the phrase “Fuzzy Wuzzy Angels” and a debt this country has never quite known how to repay.
The men in that photograph have now passed on. Their grandchildren and great-grandchildren are still on the track. They still cut down trees, lash logs together, and carry Australians who cannot walk. The continuity is not metaphorical. It is operational.[iii][iv]
The aeromedical helicopter was heard at least half a dozen times during the 2026 CWT team trek. Its sound meant that, for some casualties, in some weather and locations, the timeline from injury to definitive care had collapsed from days to hours.
It did not mean the timeline had collapsed everywhere. Where the canopy is thick, the weather is volatile, or the landing zone is two ranges away or non-existent: the timeline reverts. It reverts not to 1990 or 1980, but to 1942 – to stretcher relays, to the pace of human carriage on bad ground, to the casualty's clinical course unfolding over hours and days instead of minutes.
The lesson is the one expeditionary health planners need to keep relearning: rotary-wing extends reach but does not eliminate the gap. Any aeromedical evacuation plan, deployable hospital concept, or expeditionary health doctrine that assumes the helicopter will always come is a plan that has not walked the ground.
The men of 1942 understood this with a clarity modern forces have to work to recover. Their evacuation system was the locals, the stretcher, and the pace of the human body moving through the mountains. The modern system usually is not – until the weather closes in or the ridge is wrong, and then suddenly it is, and the question becomes whether planners accounted for the gap, or only for the helicopter.
Disease Prevention
Disease and non-battle injury (DNBI) shaped the Kokoda campaign as profoundly as any tactical decision. Across the New Guinea fighting, non-battle losses regularly exceeded battle casualties – in some periods by ratios that would today be considered campaign-ending. Malaria, dysentery, scrub typhus, dermatological infections, foot conditions, and the slower attritional toll of caloric deficit and exhaustion combined to remove more Australians from the line than Japanese fire did.
The disciplined use of chemoprophylaxis and vector-control measures developed during the Pacific War, alongside improvements in nutrition, sanitation, and casualty management changed what was operationally possible.[v]
Across the trek, the CWT team encountered, among them: electrolyte dysfunction, dehydration, heat stress, hypoglycaemia, prickly heat, golfer's rash, gastrointestinal upset, musculoskeletal injuries, friction wounds, blisters, and the early stages of trench foot. None of this is a battle injury, but all of it removes capability from a team.
The group took antimalarial tablets daily and slept under protection where conditions allowed. None developed malaria. Several developed mild gastrointestinal illnesses, managed conservatively, with none requiring evacuation. The contrast with 1942 lies in the places where modern advances have most clearly transformed the picture, but the broader inventory of disease and non-battle injuries was extensive, predictable, and exactly what the diggers had also faced.
The lesson is twofold. First, chemoprophylaxis, vector control, and the broader DNBI prevention framework do indeed work, and the chain of command that ensures compliance is genuinely force-preservation work even when it feels administrative.
Second, the underlying environmental risk has not changed – the mountains still hold the mosquitoes, the watercourses still carry pathogens, the terrain still produces the same friction injuries, foot conditions, and musculoskeletal load casualties it produced in 1942. Modern prophylaxis is a mitigation rather than an elimination, and the modern doctrine that treats DNBI as a secondary planning consideration is repeating a 1942 underestimation with better tools. In any future operation in a country like this, DNBI may well again be the largest category of loss.

The Clinician in the Group
Captain Geoffrey Hampden "Doc" Vernon was a 60-year-old First World War veteran, deafened by a shell at Gallipoli and eligible for civilian evacuation when war came to Papua in 1942. He chose to stay. He put his age down by eight years to enlist, was attached to operations supporting the 39th Battalion as medical officer for the Papuan carriers, and walked the Kokoda Track, attending to Australian soldiers and Fuzzy Wuzzy Angels alike.
He triaged casualties, performed surgical procedures, and tended to the dying in makeshift huts and jungle clearings, sometimes under enemy fire and within mortar range. He was one of the last to leave the Kokoda Plateau during the withdrawal, staying back to help the wounded.[vi]
What Doc Vernon was doing on that track was not solely clinical. The men he treated were demonstrably better off for the medicine he provided, but the historical record is consistent that he was also something else to them – a fatherly figure, a calm presence, a man whose deafness meant he could not hear the rumours that travelled along the line and whose attention could therefore be more reliably given to the man in front of him. He treated Papuan carriers with the same care he gave Australian soldiers, and that fact alone shaped the relationships on which the entire evacuation system depended.[vii]
A clinician embedded with a small team in an austere country does clinical work. The low sodium case, the strapped knees, the foot inspections, the wound dressings – these are real, and they matter. But they are not the only thing the clinician does, and arguably not the largest thing.
The team knows someone is watching. They know that if their knee goes, or their stomach fails, or they make the kind of small mistake that compounds in this terrain, there is a clinician in the group whose role is to respond. That knowledge changes how the team functions. It changes what they are willing to attempt. It changes how they sleep. That presence is itself a capability.
By the later days of the CWT trek, the trekkers had begun managing minor injuries themselves and treating the porters' complaints under the clinician's general supervision. The clinical queue thinned; the team did not. This is the form the capability takes when it works: the embedded clinician's presence eventually creates the conditions for partial redundancy, and a team that has watched a clinician work for long enough begins to do some of the clinician's work themselves.
Modern doctrine describes embedded clinicians in terms of clinical scope, equipment, evacuation timelines, and casualty estimates. These are the right things to describe. They are not the only things.
The clinician on a small team is also a node of confidence, a teacher, and a designated advocate for the body of every soldier in the group. Doc Vernon understood this. The argument worth making to modern planning is that a clinician embedded with troops in a country like this is doing more for the team than an equipment list will ever capture.
The Continuity
The Kokoda campaign is not entirely closed. The bones of Australian and Japanese soldiers are still being recovered. Unexploded ordnance is still being cleared.
The track is not a memorial site so much as a working landscape on which the past is still being settled – and on which the lessons of expeditionary health, plainly read, are still being taught.
The categories of problems have not changed in 84 years. Hydration also means sodium. Sustainment is force preservation. Foot health is a clinical intervention. Rotary wing extends reach but does not eliminate the gap. DNBI is the largest category of loss in operations like this. The clinician's presence is itself a capability. These are not new lessons; they are recoverable lessons, for any modern force willing to walk the ground and meet them.

Acknowledgements
The author would like to acknowledge and thank Brett McElwaine, Clinical Nurse, and Major Paul Dunbavin OAM, Trust Executive Officer of the Commando Welfare Trust, for their peer review and feedback on the clinical and historical content. Their contributions strengthened the piece considerably; any errors that remain are the author's own.
About the Commando Welfare Trust
This article reflects on a Commando Welfare Trust fundraising expedition along the Kokoda Track in April 2026. The Commando Welfare Trust provides emergency and long-term financial support to Australian Special Operations Command soldiers, veterans and their families. Donations are tax-deductible and all public donations go directly to beneficiaries. More information is available at commandotrust.com.
Still Interested?
For more on the historical context of this campaign, read Australia's Kokoda Campaign on The Cove.
End Notes
[i] Commando Welfare Trust, ‘About the Trust’, commandotrust.com, accessed May 2026.
[ii] Cited in P. Brune, Those Ragged Bloody Heroes: From the Kokoda Trail to Gona Beach 1942, Allen & Unwin, Sydney, 1991. See also Australian War Memorial collection records relating to Captain T. Grahamslaw, ANGAU.
[iii] G. Silk, Pte. George C. ‘Dick’ Whittington led by Raphael Oimbari, photograph, Buna, Papua New Guinea, 25 December 1942, Australian War Memorial collection.
[iv] The phrase predates the photograph. H. (‘Bert’) Beros wrote the poem ‘The Fuzzy Wuzzy Angels’ in October 1942, first published in The Courier-Mail, Brisbane, 31 October 1942.
[v] A. S. Walker, The Island Campaigns, Australia in the War of 1939–1945, Series 5 (Medical), Volume III, Australian War Memorial, Canberra, 1957; Department of Veterans’ Affairs, ‘Australia’s War 1939–1945: Kokoda’, Anzac Portal, anzacportal.dva.gov.au, accessed May 2026.
[vi]Australian War Memorial, ‘Vernon, Geoffrey Hampden’, People profile, ID P11029120, awm.gov.au, accessed May 2026; P. Brune, Those Ragged Bloody Heroes.
[vii] Vernon’s observation appears in his wartime diary. The relevant passage reads, in part: ‘being very deaf, from concussion deafness on Active-Service 1915 I do not gather much information from others I therefore miss much that goes on including the many rumours and false reports that constantly passed along the line. The absence of these may be an advantage’. Diary held in the Australian War Memorial collection. See also Australian War Memorial, ‘Vernon, Geoffrey Hampden’, People profile, ID P11029120.




