




Large-scale combat operations (LSCO) against near-peer adversaries (NPAs) will undeniably have large-scale casualties. LSCO will involve tactics and weaponry not seen in the GWOT era of operations. NPAs will be equipped with accurate, advanced, long-range weaponry and electronic warfare capabilities, including jamming. This constricts the evacuation chain methods, particularly air assets, and results in delayed definitive medical and surgical care. NGOs such as Global Surgical and Medical Support Group have already begun to experience similar difficulties in the Russo-Ukrainian conflict. They have noted issues with zero notification casualties caused by limited communications, regular mass casualty numbers, and questionable safety of medical resources (Epstein et al. 2023).
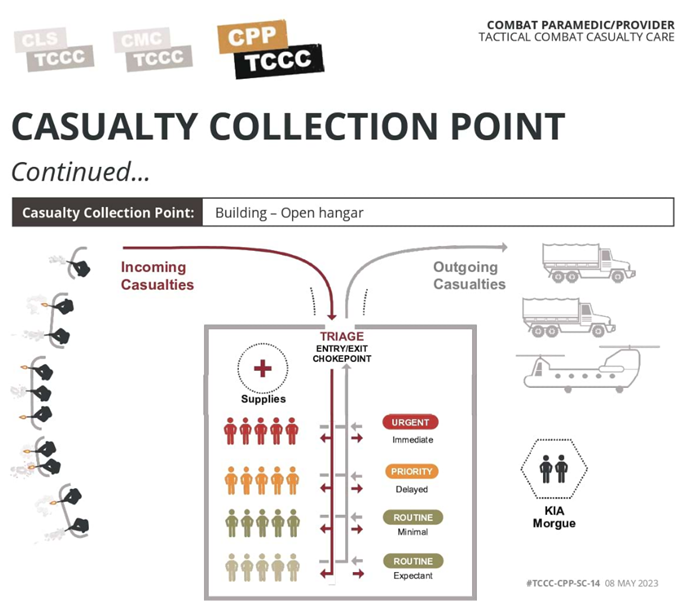
Casualty collection points (CCPs) are often hastily put together medical management facilities near front-lines used to quickly and efficiently gather casualties, conduct lifesaving interventions, and position casualties for higher levels of medical care (TCCC Guidelines). CCPs can be medically or non-medically staffed based upon the assessment of risk versus the availability of personnel (ATP 4-02.2). CCPs will be heavily employed in LSCOs. CCPs can experience mass casualty traffic during high-tempo operations. These incidents overwhelm triage, leading to patient backlogs which tie up front-line personnel who are stuck bringing casualties to the CCP. Traditional CCP setups, particularly those reliant on tents, lack the flexibility and responsiveness needed to adapt to rapidly shifting fronts.
To address these limitations, there needs to be an exploration of a vehicle-based CCP system. This concept revolves around a rapidly deployable team, designed to assist in the management of mass casualties. It would allow for quick establishment, collapse, and relocation of CCPs. This allows quicker set up, resulting in patients being accepted quicker and earlier patient management causing reduced traffic backlog. This could also be sent forward from a holding position to supplement a snap CCP. Ideally, there would be two teams. This is split into an “Active Section” in an established CCP, engaging in current casualty management. As this CCP is overwhelmed or the front moves the second section is employed. The second “Mobile Section” is collapsed and ready to establish a new CCP or reinforce another CCP location as needed. This dual callsign approach ensures continuous operation whilst maintaining flexibility to respond to evolving situations.
A vehicle-borne CCP is focused on a single vehicle that would be designed as a triage vehicle. All CCPs require a triage point, which allows controlled, concise movement of casualties. Positioned at the entry point of the CCP, this vehicle handles the initial triage and acts as a physical marker of the triage point. It serves as the first contact point for incoming casualties and facilitates immediate sorting based on casualty severity. Whilst being open, this triage could be enhanced with environmental protection by setting up a tarp between two vehicles or to surrounding features. This design eliminates reliance on portable tents, favouring a more manoeuvrable and terrain-adaptable solution. A vehicle-borne CCP can also carry significantly more equipment than a small section can. In an operational space where EW hinders or eliminates radio traffic, casualties will arrive unannounced and potentially in large numbers. A large breadth and number of stores will be required to allow CCP operators to remain effective and allow efficient resupply to teams moving to and from the CCP.
The CCP vehicle itself needs to be ergonomic to the users and allow easy access to supplies. The current ambulance is unsuitable for this concept due to limited additional medical supply storage and restricted patient access inside the ambulance. This restricted access prevents 360-degree patient assessment and care. Instead, the proposed platform is a G-Wagon carry-all variant, colloquially referred to as the "ute", with shelved medical bins on the tray. These medical bins would face out, allowing access without removing the whole bin. These tubs should be removable to facilitate relocation and reallocation of stores. By placing the bins on both sides of the tray facing out, you gain a central storage area on the tray. This area is useful as a larger storage area for stretchers, litter stands, and other required long or cumbersome equipment. This configuration offers several advantages, including terrain adaptability, ergonomics, and modularity. These vehicles can navigate confined terrain where larger vehicles cannot. The lower tray height in comparison to the 40M truck or Hawkei cargo variant allows easier access to the equipment without removing the bins. The use of the side access bins allows for quick modification for different incidents. The vehicle could be quickly changed from a CBRN incident loadout to respond to a conventional artillery strike on a convoy by switching out the bins.

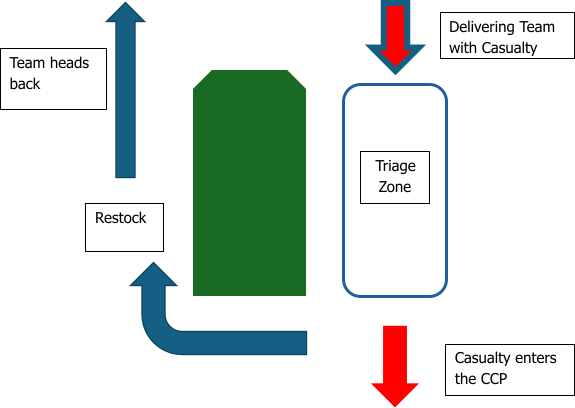
When employed, the casualty flow should be simple. The casualty arrives at the driver's side of the triage vehicle with the delivering team placing the stretcher on the litter stands. The medical team conducts rapid triage and any necessary interventions. The delivering crew peels around the back of the vehicle to restock from the other side of the vehicle and return to the front-line. Casualty is moved into the respective casualty area and monitored, transferred to a resuscitation area to be stabilised or moved rearward to the next appropriate facility, e.g. Role 2.
There is the potential to expand on the triage vehicle concept. As this concept moves forward, the next part would be the development of a Resuscitation Bay crew. This is formed by the second and third vehicles parked side-by-side a few meters apart. Medical tubs on the outer sides of these vehicles remain closed for restocking and transport, while inner-facing tubs provide access to critical supplies needed in a resuscitation bay. A tarp strung between the vehicles offers environmental protection and visual concealment. If needed, the CCP setup can be transitioned indoors, either using portable tubs removed from the back of the vehicles or the same setup but inside a hangar. This would create a 3-car packet, allowing the callsign to operate similarly to a cavalry troop.
While a potentially effective answer to some of the issues faced by CCPs in an LSCO, this system has trade-offs. A vehicle has an increased footprint and higher resource demand than current hastily put-together CCPs. The proposed vehicles are soft-skinned and offer limited ballistic protection.
LSCOs against NPAs will require a new understanding of mass casualty patient evacuation within a severely constrained environment. It will require a high level of adaptability and innovation. Whilst this vehicle borne CCP concept is not an elixir, its introduction aids in answering issues faced by medical teams in the current LSCO.





These need to be slick and well practiced drills as casualty management and delay is often induced when everyone rushes in trying to help and adding more chaos to an already chaotic situation. I think a key benefit to your ideas is the control offered. I'd also add that the NCOs leadership here is vital, be it the Lance Corporal section 2IC managing the casualty at the point if injury, the platoon Sergeant clearing and back loading the casualty; or the Company Sergeant Major coordinating the company casualty collection and exchange point. It is always the calm hands of experienced NCOs that help reduce the chaos, especially in casualty management.
Thank you for your article, and for the time you have taken in considering this idea to improve battlefield casualty management!