




“The resulting operational environment, known as large-scale combat operations (LSCOs), will increase the scope of wounded service members to levels not seen since World War II (WWII).”[1]
Australia faces its most challenging strategic environment since World War II and the threat of large-scale combat operations (LSCO). Whilst the nature of war remains a violent clash of wills, the character of war continues to evolve with more advanced weaponry, long range strike, drone attacks, hybrid warfare and subversive tactics. The Russia-Ukraine War is seeing modern anti-tank munitions achieving close to 75% fatality used asymmetrically along with incendiary munitions designed to burden medical and evacuation chains.[2] With the increased threat picture and predicted higher casualty rates in LSCO, effective C3, health planning, treatment and Casualty Regulation (CASREG) is required to ensure survivability. To prepare our people for the casualties expected in LSCO, 3 Brigade should focus on three main areas for medical training throughout 2025.[3] Firstly, POI care and evacuation to integral health capabilities. Secondly, prolonged field care at both the POI and Role 1, and finally C3 throughout this process to ensure timely reports and returns to enable effective CASREG.
Casualties in the Russia-Ukraine War are commensurate with several major campaigns in WWII with 850 casualties per day across both nations and civilians.[4] For a small Army such as ours, estimates commensurate with these would be catastrophic. With health planning and CASREG stagnating in the Australian Army since it was last reviewed holistically on Exercise Talisman Sabre 2019,[5] we must take every opportunity to include medical training on the road to war exercise series in 2025, or risk culminating in the early days of conflict.
Timely and effective treatment at the Point of Injury (POI) saves lives, proven in recent conflicts in Iraq and Afghanistan, with Tactical Combat Casualty Care (TCCC) as the first stage within the Land Based Trauma System (LBTS).[6] This is achieved largely through the control of haemorrhage; however, LSCO will extend the lines of communication that will impact the ability to rapidly evacuate personnel requiring surgery, resulting in the need for forward blood and surgical capabilities to save lives. Evacuation from POI to the integral Role 1 is the responsibility of the battlegroup, thus regular training between health FE and the battlegroup will enhance the understanding of SOPs/TTPs for forward evacuation.[7] TS19 identified a paucity of surface evacuation platforms and RWAE as requiring attention, which has not changed.[8] With 16 allocated ambulances within 3 Brigade's UE, units must get creative with the use of opportune CASEVAC platforms.[9] Every opportunity should be used to integrate with enablers to inculcate all FEs understanding of treatment and evacuation within their remit, inclusive of an understanding that the CASREG cell (CRC) co-ordinates tactical evacuation from the battlegroup's R1.[10] Notably, this does not mean we should dismiss opportunities to evacuate to surgical care as soon as practical – this should always be the aim as it save lives, but as is being seen in Ukraine, it is not always immediately achievable.
The ‘golden hour’ or 10-1-2 is unrealistic in LSCO and whilst we need to address the ability to evacuate through a paucity of surface platforms, we must prepare our people to hold casualties for prolonged periods, something we hold the levers to now. Britain adopted the ‘golden hour’ from experiences with casualties during the Falklands War,[11] an example of how processes were enhanced through contemporary experience, and whilst this saves lives, fighting in the Ukraine is seeing POI care extending over 12 hours requiring adaptation once more.[12] Anecdotes of 11 hour+ evacuations during Ex Talisman Sabre 24 were circulated and used to highlight sub-optimal performance, but could be largely symptomatic of our expectations of rapid evacuation as experienced in the Middle East. LSCO may see extended evacuation as the norm, thus 3 Brigade can prepare for this by ensuring TCCC as part of Combat Behaviours is trained regularly, 3 Brigade in collaboration with 4 HB train an appropriate number of CFAs (to Pl level as a start point), and prolonged field care is incorporated into collective training during the design phase. Ex POZIERES lessons in Oct 24 is an opportunity to set the conditions for this into 2025. Forward blood and mobile surgical capabilities also enhance survivability and are bodies of work being ‘fast tracked’ – incorporating information sessions and serials into training next year can set the conditions for reality as soon as possible.[13]
Finally, CASREG ensures casualties are evacuated to the most appropriate health facility, minimising handling where possible. C3 remains central to this and ensuring each echelon is well-versed in their responsibilities for reports and returns is fundamental. Degraded communications, as seen in Ukriane, also means we need to be well-versed with other alternatives such as Signal groups and voice over BMS systems that not all have access to. As part of early integration in 2025, aligning 4 HB capabilities to battlegroups and having a deep and instinctive understanding on how call signs communicate, will enhance the efficiency of transferring the right information at the right time to effect evacuation. This can be further enhanced through updating 3 Brigade SOPs including the graphic depiction of roles and responsibilities throughout the LBTS and the C3 methods available. Deliberate health planning throughout will also ensure grouping and re-grouping of health assets to the main effort provides the greatest survivability options to commanders and maintaining a fighting force.
LSCO will result in increased casualties, but we have the levers to enhance our survivability through greater integration and improving our understanding of SOPs/TTPs. Future wars will see casualties being held at the POI or R1 longer and evolving capabilities such as forward blood, forward surgical capabilities and the increased capacity for clinicians to provide prolonged field care, will save lives. We should always seek to evacuate as rapidly as the situation allows but must include deliberate medical serials within our training that challenges decision-making, imposes dilemmas at all levels of the LBTS, forces our people to hold for longer periods, be creative with evacuation platforms and challenges decision making. A fit fighting force relies on it.
SHO 3 Brigade – observations from EX BROLGA RUN 2024.
The information below is based on diary entries, AARs post major events and observations throughout the exercise, including working with and being mentored by Brigadier Georgina Whelan. Each major medical scenario involved an AAR with Brigadier Whelan from the information I had available within Delta Node and communications with the SO3 Health in Alpha Node.
Health Capabilities
- Assignment of 2 BDE sFE across multiple tasks.
- R1s doctrinally have two x Treatment Teams (TT) and a holding capability.
- BGs seek to quickly evacuate casualties based on 10-1-2 or golden hour thinking and so manoeuvre is not inhibited as the TT has limited ability to hold casualties.
- BGs seek to quickly evacuate casualties based on 10-1-2 or golden hour thinking and so manoeuvre is not inhibited as the TT has limited ability to hold casualties.
- TS25 – If strategic environment allows, synchronise OAA/Is to enable maximum health capabilities ISO TS 25 to enable two x TTs where possible and ability to hold casualties.
- Seek to have ME with the flexibility of two x TT and staging/holding capability
- Seek to have ME with the flexibility of two x TT and staging/holding capability
- R1s doctrinally have two x Treatment Teams (TT) and a holding capability.
POI care and evacuation
- There were several examples during the Ex where personnel were evacuated directly to the R2F attached to 3 CSSB without CASREG authority.
- Potential to overwhelm a limited surgical effect early in a phase and place unnecessary constraints on the system.
- Go back to first principles during WALK series to ensure each echelon has an understanding of LBTS and the levers to evacuate casualties to the next level of care. Inclusive of C3 systems which each BG uses to provide reports and returns.
- Go back to first principles during WALK series to ensure each echelon has an understanding of LBTS and the levers to evacuate casualties to the next level of care. Inclusive of C3 systems which each BG uses to provide reports and returns.
- Potential to overwhelm a limited surgical effect early in a phase and place unnecessary constraints on the system.
- LBTS – OBJ Bear clearance – Casualties made it to BG CCP but no further rearward which by itself is not a concern, but no conclusion to serial was evident.
- Engagement with CTC to plan deliberate serials over dated casualty cards that trigger an action with no OT following the serial through to conclusion.
- D Node had two IDF serials where OTs provided casualty cards and then had no further engagement, providing limited training effect for the R1 TT they were evacuated to. OTs should be in a position to provide updated MISTs and realism to enhance this for LSCO.
- Engagement with CTC to plan deliberate serials over dated casualty cards that trigger an action with no OT following the serial through to conclusion.
- Battlefield discipline - NO DUFF MEDEVAC - patience, send R2s, do not commence evacuation out of your AO/Ech prior to CASREG function to ensure casualty is evacuated to the most appropriate facility.
- Lack of discipline for NO DUFF Pri 3s which are not an emergency. Units wanted to get people off range immediately and in nearly 50% of instances, not waiting for CASREG coord.
- I assess this is a product of how we do unit training at TFTA and lack of medical assets to hold casualties that are not urgent for evac. We need to get units comfortable holding casualties that are not medically urgent.
- I assess this is a product of how we do unit training at TFTA and lack of medical assets to hold casualties that are not urgent for evac. We need to get units comfortable holding casualties that are not medically urgent.
- Lack of discipline for NO DUFF Pri 3s which are not an emergency. Units wanted to get people off range immediately and in nearly 50% of instances, not waiting for CASREG coord.
- Evac platforms, MEDEVAC and CASEVAC along with SOPs/TTPs for evacuation.
- Need to get better in planning around creative solutions for sitting/walking casualties.
- BG conducts forward evac through use of integral ambulance (MVP 2-3 x ambulance per BG) to POI and back to assigned R1.
- CCP sighted in proximity to R1 to allow CSST (or RWAE if available) to conduct tactical evac to next level of care (MVP for CSST is four x ambulances, generally from 4 HB).
- CCP sighted in proximity to R1 to allow CSST (or RWAE if available) to conduct tactical evac to next level of care (MVP for CSST is four x ambulances, generally from 4 HB).
- Need to get better in planning around creative solutions for sitting/walking casualties.
C3 and Reports/returns
- Two serials of 3-4 x Pri 1s that had not made it to a TT or R2F after 7 hours and were subsequently KIA.
- Lack of R2s did not provide CRC information to regulate or achieve optimal outcomes for casualties.
- 9L and MIST improved markedly Ph2B
- Casualty priority v triage priority Pr 1,2,3 (Cat A,B,C ) Pri 1 No signs life, no such thing as Pri 4
- Use of PMKeys with MISTs enabled quick ID of casualties.
- 9L and MIST improved markedly Ph2B
- LSCO may see this as the norm, but the inclusion of the serials to test that effect is required, including OTs following the casualties so we don’t decide to end a valuable learning opportunity due to lack of information.
- Lack of R2s did not provide CRC information to regulate or achieve optimal outcomes for casualties.
- Command and control relationships – greater integration and work required on the use of R2F. Mixed messaging on where it should be placed and who owned it at various times.
- Greater guidance required in orders, HSP, sync matrix and TASKORD matrix on the types of tasks - BPT, O/O and NB or NLT timings.
- Greater guidance required in orders, HSP, sync matrix and TASKORD matrix on the types of tasks - BPT, O/O and NB or NLT timings.
- Node construct options for effective CASREG – discussed with 4 HB and supportable COA is: 4HB provide CRC effect in A node and 3X SO3 Hlth in B node conducting planning.
- Where NCS may change for a longer period of time, we need to have at least 2 people to cover 24 hr Ops in CRC function to enable CASREG.
- Where NCS may change for a longer period of time, we need to have at least 2 people to cover 24 hr Ops in CRC function to enable CASREG.
End Notes
[1] Remondelli, Mason H., et al. “Casualty care implications of large-scale combat operations”. Journal of Trauma and Acute Care Surgery 95, no. 2S (2023): S180-S184.
[2] Epstein, Aaron MD, et al. “Putting Medical Boots on the Ground: Lessons from the War in Ukraine and Applications for Future Conflict with Near-Peer Adversaries”. Journal of the American College of Surgeons 237(2):p 364-373.
[3] Notwithstanding parallel efforts to advance our forward blood and surgical capabilities.
[4] Remondelli, Mason H., et al. “Casualty care implications of large-scale combat operations”. Journal of Trauma and Acute Care Surgery 95, no. 2S (2023): S180-S184.
[5] BR1906821, JWS 2019: Evaluation Report – LBTS Ex TALISMAN SABRE 2019 (attached).
[7] Forward Evacuation – the evacuation of a casualty from the initial POI to the first HF within the AO (BG R1 in this instance).
[8] BR1906821, JWS 2019: Evaluation Report – LBTS Ex TALISMAN SABRE 2019 (attached), pg 6
[9] CASEVAC – Nonmedical evacuation (Ukraine are using train carriages refitted with hospital beds)
[10] Tactical Evacuation – the evacuation from one health facility (BGs R1) to another health facility in the AO
[11] Batty, Charles G. "Changes in the care of the battle casualty: lessons learned from the Falklands campaign." Military medicine 164, no. 5 (1999): 336-340.
[12] Email – CHATREP with Australian fighting in the UKR Jun 2024.
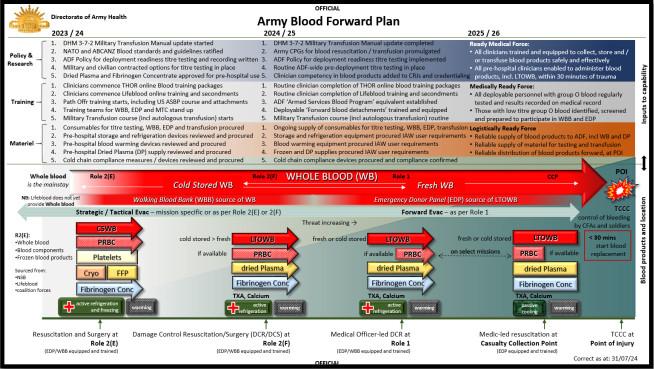
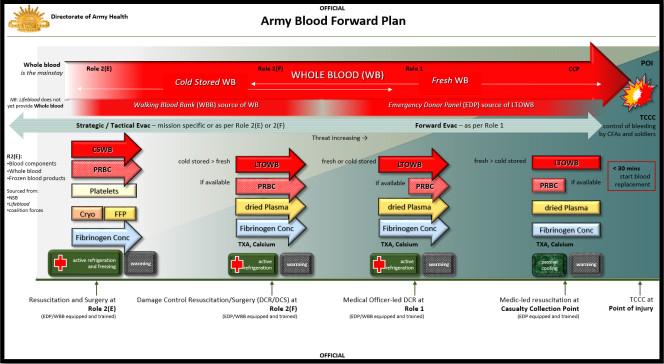
[13] See infographic courtesy DAH, AHSWG 23 Aug 24 – page 3.




